Most however are placed in the stomach. The wire was left in.

Iatrogenic Bronchopleural Fistula From A Dobhoff Tube Radiology Case Radiopaedia Org
The patient was found dead.

. It is also important to note that feeding tube insertions causing pulmonary complications are not always related to tracheobronchial insertion. We had a situation where a dubhoff did not show up anywhere on the x-ray. The tip sits below the diaphragm.
After insertion correct placement in the body is usually checked with the help of X-rays or fluoroscopy. With CORTRAK 2 you. Therefore bilateral chest tubes were placed.
Dobhoff tubes DHT are narrow-bore flexible devices that deliver enteral nutrition for critically ill patients. A DHT was inserted after intubation for feeding purposes. However in our patient who had history of Roux-en-Y the DHT bypassed the duodenum and.
An electromagnetic stylet provides real-time location information on the tube tip placement within a patients anatomy. Dobhoff tube is a special type of nasogastric tube NGT. After removal of the tube a follow-up chest x-ray revealed iatrogenic bilateral pneumothoraces.
Thus DHT insertion requires radiologist confirmation of correct placement with chest x-ray CXR increasing clinical delays. The tube is inserted by the use of a guide wire called the stylet see image1 which removed after the tube correct placement is confirmed. The x-ray was read and placement confirmed.
Placement of the tube is checked by a post-insertion radiograph centered on the. A Dobhoff tube was placed by a house physician. It was a 12 french by the way.
Tube descends the thorax in the midline. Follow-up abdominal x-ray revealed displacement of the Dobhoff tube in the left pleural space. Normally the DHT tip should be placed in the 2 nd to 3 rd portion of the duodenum and would create a C-shaped tracing on the X-ray.
Tube feedings were initi-ated. As seen in Figure 1 the tip of the Dobhoff tube is in the left mainstem bronchus. Aspiration and a Dobhoff tube was subsequently placed at the bedside for delivery of enteral nutrition.
After removal of the tube a follow-up chest x-ray revealed iatrogenic bilateral pneumothoraces. Tube feedings were begun. Confirmed placement af-ter reading the x-ray.
At our facility we x-ray all feeding tubes for placement verification. Place tube through nares and ask patient to swallow as you pass the tube. Department sought to change the Dobhoff NG tube insertion practice to reduce the number of tube placements within the airway.
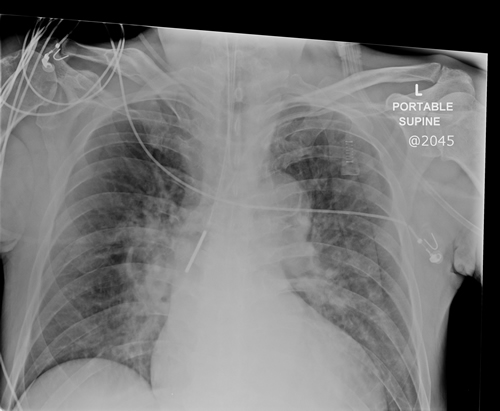
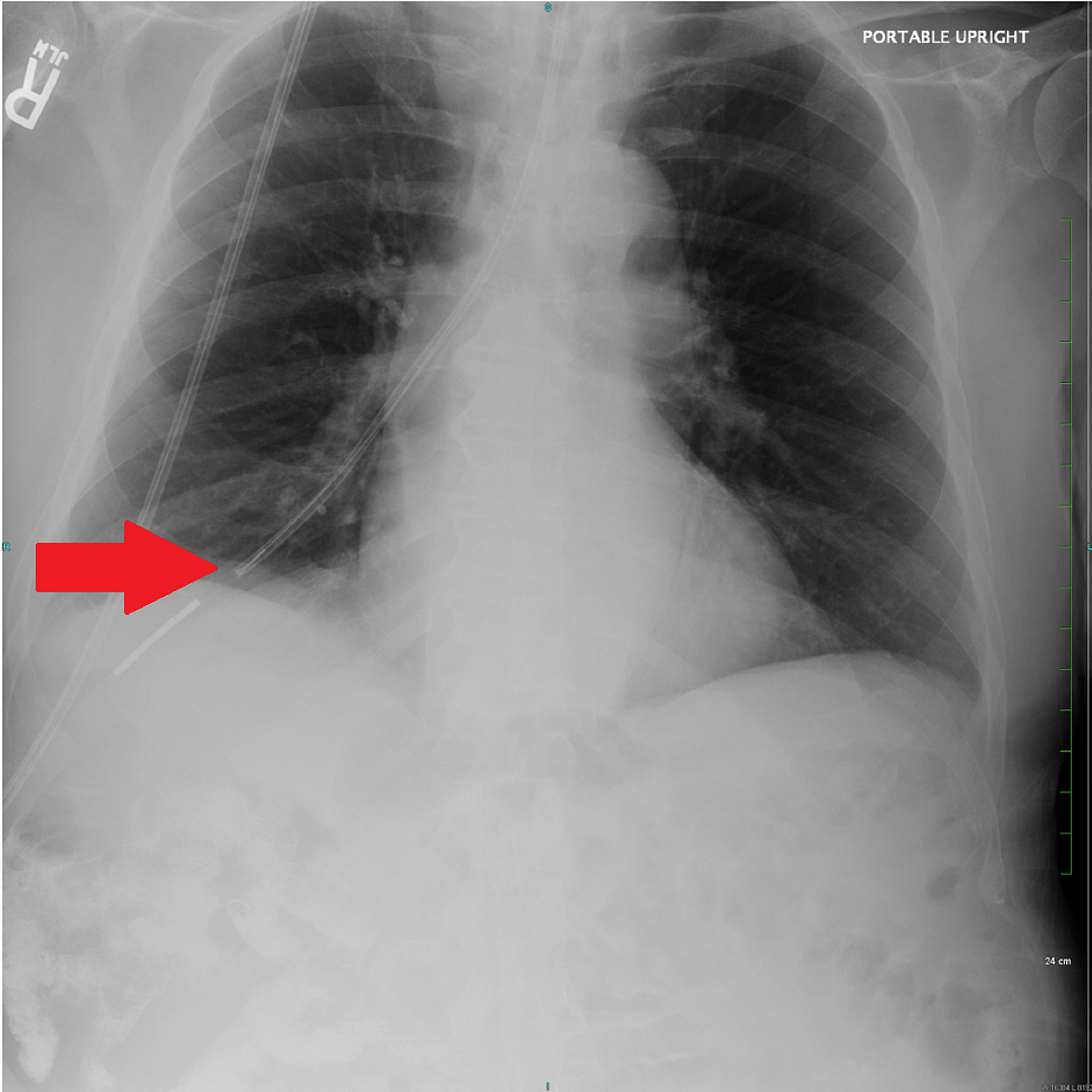
Dobhoff tube is a special type of nasogastric tube NGT which is a small-bore and flexible so it is more comfortable for the patient than the usual NGT. A chest X-ray performed shortly after the tube placement demonstrated that the tip of the Dobhoff tube was within the right lung base following the course of the right mainstem bronchus Figure 1. The patient experi-enced respiratory dis-tress.
ZWith NG tubes placement should be obvious. The nurse is sure of gastric placement. On-screen visualization provides immediate feedback on tube placement which can reduce or eliminate the need for x-ray confirmation.
Tube feedings were initiated. Tube feedings were begun. Data was collected at initial placement prior to x-ray confirmation.
The feeding tube has a weighted metal tip and a guide wire for insertion. The practice change consisted of implementing the two-step x-ray process which entails the clinician inserting the Dobhoff NG tube to 35 centimeters cm which is at the anatomical position. We followed the two-step bedside approach that was first described in 19891 First we advanced the tube to 30 centimeters and took a chest x-ray.
Most tube positions are checked by assessing pH of tube aspirate. Most however are placed in the stomach. The patient was found dead.
The Dobhoff tube was introduced in the mid-1970s by surgeons Robert Dobbie and Jim. Two-step approach with a portable chest x-ray to assess accurate and safe placement. A review of the x-ray showed that the feeding tube was in the main bronchus.
Tube bisects the carina. Nasoduodenal ND feeding tube placement is a procedure in which an x-ray monitor is used to guide the placement of a soft feeding tube through the nose into the small bowel duodenum. CORTRAK can be used to confirm bedside tube placement without x-ray.
A Dobhoff tube was placed by a house physi-cian. Keeping this in view how do you check the placement of a Dobhoff tube. If we had continued.
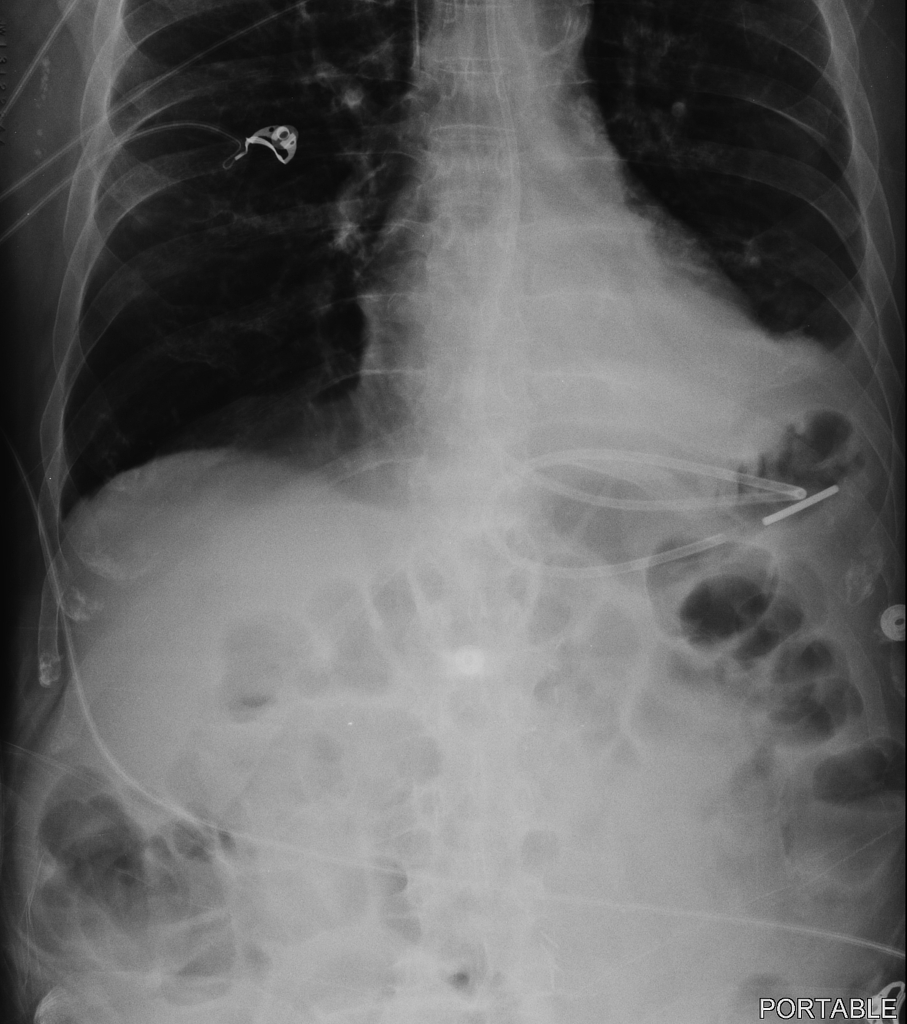
ND feeding tubes may be used for long-term enteral nutrition. Follow-up abdominal x-ray revealed displacement of the Dobhoff tube in the left pleural space. Abdominal x-ray after fluoroscopic guided Dobhoff tube placement.
The patient experienced respiratory distress. An abdominal X-ray was obtained to confirm placement of the DHT Figure 1. We told the nurse to check by air bolus while we await a second xray to be completed and read.
Tracheobronchial insertion of DHTs presents a significant risk for pulmonary complications. Tip of feeding tube should be in 2nd or 3rd portion of duodenum. When tube is connected to low intermittent suction there should be return of gastric contents If there isnt confirm placement with xray KUB zWith dobhoff tubes should always confirm placement as no suction will be applied.
Small amount of contrast injected to confirm Dobhoff tube see arrow positioning in the fourth portion of the duodenum. Auscultation was performed in all 78. What can go wrong.
Dobhoff tubes come with a radiopaque stripe making them easily visible in. Due to the limitations of bedside techniques in confirming Dobhoff tube placement x-ray remains the gold standard in confirmatory testing 1910. Measure tube from tip of nose to subxyphoidprocess about 3035cm in most patients Step 2.
Most tubes are visible on a chest x-ray without a guide wire. The x-ray was read and placement confirmed. Tube crosses the diaphragm in the midline.
Patients are usually positioned on the right side while the tube is put into the nose. Steps for NG Feeding Tube Placement in an Awake Patient. An x-ray can ensure that the Dobhoff tube has been placed correctly.
Feeding tube with guidewire brown tip that is 120cm preferred over blue tip dobhoff tube Lubricant 60 ml syringe. The side hole is usually located just proximal to the tip. Placement of the tube is checked by a post-insertion radiograph centered on the.
A review of the x-ray showed that the feeding tube was in the main bronchus. Of 78 nasoenteral intubations in 46 patients using a Dobbhoff Biosearch Medical Products weighted enteral feeding tube gastric aspirates were evaluated in 28. ZEndotracheal placement zEpistaxis zSinusitis.
In order to prepare a patient for the insertion of a Dobhoff tube the esophagus and nasal cavity are numbed and the patient if conscious may be given a mild sedative. Acute hypoxemic respiratory failure ensued. Tip of feeding tube should be in 2 nd or 3 rd portion of duodenum.
You need to be confident that you can see the tip. The physician confirmed placement after reading the x-ray.
Procedure Insertion Of An Oral Nasal Small Bowel Feeding Tube Lhsc

Procedure Insertion Of An Oral Nasal Small Bowel Feeding Tube Lhsc

Abdominal X Ray Revealing The Dobhoff Tube Traversing The Left Main Download Scientific Diagram
Icu Chest Radiography Lines Ng Dobhoff Etc Youtube
Dobhoff Nasogastric Tube Tube Radiology Case Radiopaedia Org
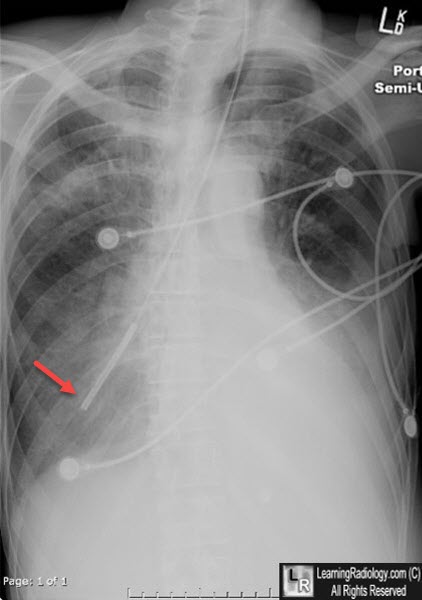
Learningradiology Dobhoff Dobbhoff Tube Malplaced Rll
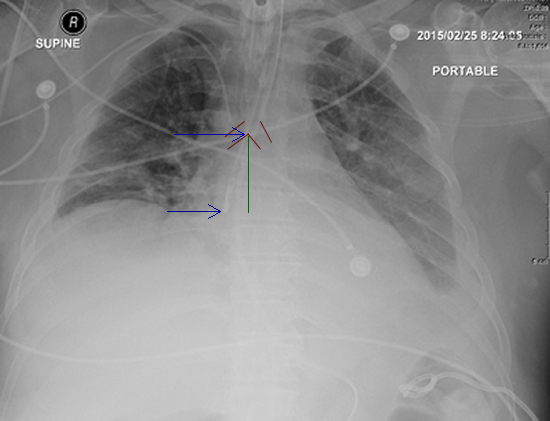
Cureus Hemothorax Following Traumatic Dobhoff Tube Insertion
Procedure Insertion Of An Oral Nasal Small Bowel Feeding Tube Lhsc
0 comments
Post a Comment